There is no American institution more dedicated to collective action than our armed forces. Even a cursory examination of our Medal of Honor winners shows how the good of the collective triumphed over the well-being of the individual. Many of Secretary Hegseth’s orders regarding appearance, fitness, and demeanor have easily fit within that framework – until his latest decision to remove the influenza vaccination from the mandatory inoculations required of all members.
“But we will not force you, because your body, your faith, and your convictions are not negotiable."
That decision was cloaked in the garments of medical freedom and the end of an “era of betrayal” from the “overreaching mandates” of COVID, continuing to echo the tension between autonomy and collective action for the civilian population during the COVID pandemic. The cacophony of Internet voices quickly took to their respective public health and political corners, casting far more shade than light. However, a deeper look reveals reflections worth considering. The question is not simply whether influenza vaccination is good medicine, but whether mandating it remains good military policy.
Hypocrisy or Tradeoff
 Many commentators noted that it was General Washington who first mandated inoculation, in this case against smallpox, for our troops. Roughly “90% of the Continental Army’s 70,000 fatalities from 1775 to 1781 were because of the disease.” This underscores General Washington’s concerns, which remain relevant today: operational readiness.
Many commentators noted that it was General Washington who first mandated inoculation, in this case against smallpox, for our troops. Roughly “90% of the Continental Army’s 70,000 fatalities from 1775 to 1781 were because of the disease.” This underscores General Washington’s concerns, which remain relevant today: operational readiness.
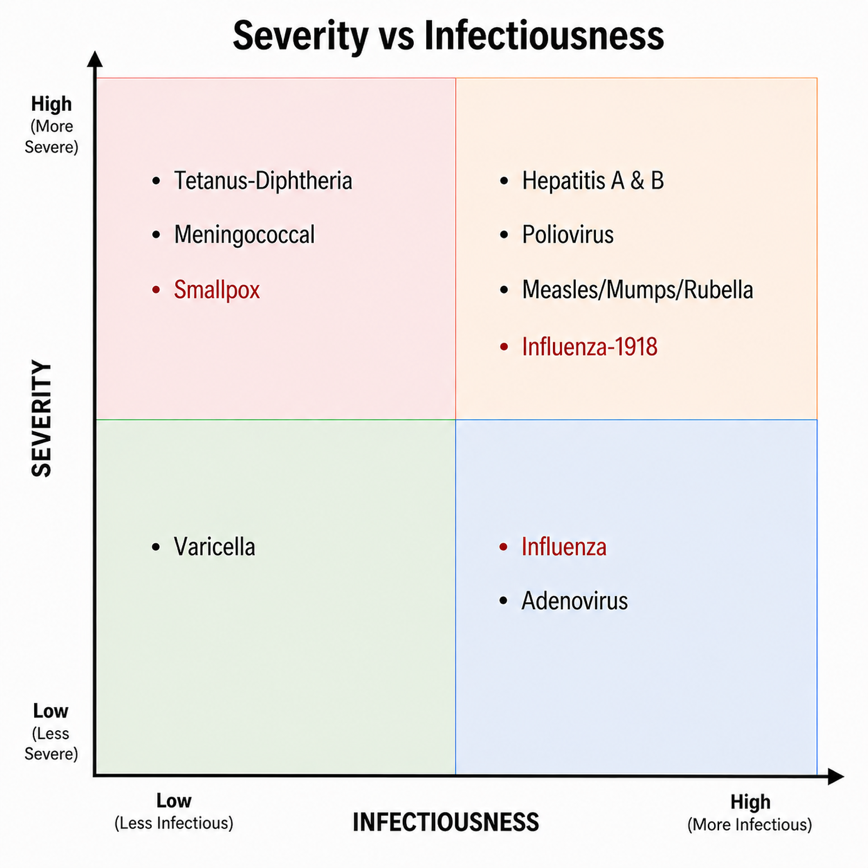
Using information on infectiousness, the R0, and the overall severity of the eight diseases formerly requiring vaccination, we produce this diagram.
Operational readiness is a function of both factors. As you can see, smallpox [1], while less infectious, causes significant morbidity and mortality; influenza, more infectious, especially in close quarters such as aboard naval vessels, has little morbidity and mortality among the armed forces demographic.
That distinction matters. The Washington comparison is rhetorically powerful, but not a full explanation. While Secretary Hegseth’s framing of the decision suggests a “blind squirrel finding a nut,” we must consider that this was, in fact, a considered tradeoff.
Some commentators framed their dismay by comparing the current situation to the armed forces’ first encounter with influenza in 1918. As you see, that earlier strain, to which we were all “naïve,” was far more severe than today’s seasonal variant, especially with respect to the demographic of concern, the young men in WWI’s armed forces. It is an apples-and-oranges comparison.
Influenza and Readiness
A review of respiratory infections in the military noted that during the 1918–1919 pandemic, about one-quarter of the American Expeditionary Forces fell ill. Overall fatality rates were about 5%. As with smallpox during the Revolutionary War, the disease ultimately caused more harm than combat: roughly 792,000 soldiers were hospitalized, and more than 57,000 died from influenza and related pneumonia, exceeding the 50,280 combat deaths in World War I. The outbreak severely disrupted operations, costing an estimated 8.7 million duty days; at some bases, such as Camp Funston, hospitalizations peaked at 150 per day.
The 2009 H1N1 pandemic also significantly affected the military. Weekly case counts in the Military Health System reached 200–300, with about 10% requiring hospitalization. Overall hospitalization rates were three to four times higher than in preceding years, underscoring the continued vulnerability of military readiness to influenza outbreaks. The review ends on this note:
“Substantial virus shedding and transmission, particularly of influenza virus and adenoviruses, may occur in persons not yet ill or with mild or subclinical infections, making routine, compulsory influenza virus and adenovirus immunizations the most important control measures available to the U.S. military today. … Prevention programs must be supported by sound epidemiological data and the constant attention of public health professionals.”
That is the strongest argument against Hegseth’s change. Influenza need not be individually catastrophic to be operationally meaningful. Its impact centers around timing and concentration: enough individuals in the same unit being sick at the same time is sufficient to impair operational readiness.
The most recent outbreak of influenza in 2014 involved the USS Ardent, a small Navy minesweeper. The crew of 126 shared a common circulating air system, spaces, and sleeping quarters, as well as surfaces like handrails and door handles. While docked in San Diego, the off-shore crew likely introduced influenza A, which was already circulating at the time. Close-quarters living then amplified the spread, resulting in 16 confirmed cases on board and a loss of 43 working days. Despite a 90% vaccination rate, the CDC ends its report by saying, “influenza outbreaks can still occur in highly vaccinated military populations.”
Another study in BMJ Military Health examined an influenza B outbreak in 2026, in which unvaccinated relief troops were integrated with vaccinated troops, resulting in an overall vaccination rate of 56%. In this instance, vaccination was significant, reducing infectiousness in the vaccinated by 83%.
These examples point in two directions. Vaccination is not a force field; outbreaks can still occur in highly vaccinated populations. However, vaccination may reduce the size and operational consequences of those outbreaks.
Secretary Hegseth raises a similar concern about the COVID mandates’ impairment of operational readiness. The comparison is imperfect but not irrelevant. COVID forced the military to confront a different readiness problem: not illness clustering within a unit, but resistance to compulsion across the force.
COVID’s Shadow
During the COVID mandate, the military had roughly 2 million active-duty, reserve, and National Guard service members. About 8,400 were involuntarily separated rather than receive the vaccine—less than 1% of the total force [2]. Yet even small losses can matter when they involve trained personnel, scarce specialties, or units where a few absences disrupt mission capacity.
In contrast to influenza outbreaks, where readiness losses are clustered, those separations were spread across time, geography, and specialty. The military is therefore weighing two different kinds of readiness loss: the distributed institutional cost of coercion versus the concentrated operational cost of illness.
The decision about the flu vaccine can be read as a post-COVID recalibration. In a high-threat setting, the collective claim over the body is easier to justify. In a lower-threat, recurring disease like seasonal influenza, the institution may tolerate more individual latitude to avoid reactivating the resistance, attrition, and legitimacy problems produced by prior mandates.
In that sense, the institution has learned that compelled medical compliance has practical limits. Influenza policy now reflects not simply a judgment about vaccines, but a substitution of risks. The tradeoff that is not explicitly addressed is this:
- Does the vaccine prevent operationally meaningful outbreaks?
- Does the mandate cause losses in critical personnel or recruitment/retention friction?
- Which risk is more disruptive to mission execution?
The Military Body
At its foundation, the military exists to achieve coordinated objectives of defense and deterrence, which require unity, discipline, and obedience to command. Individual autonomy is deliberately constrained in ways that would be unacceptable in civilian life. Orders are expected to be followed; personal preferences are secondary, and even basic freedoms of movement, speech, and appearance are regulated.
That does not mean autonomy disappears. Our military preserves limited forms of individual judgment through concepts such as “mission command,” in which commanders set the objective while subordinates retain room to adapt. Similarly, unit commanders can require influenza vaccination if, in their judgment, it hampers operational readiness in their local circumstances. Autonomy survives, but only when it serves the mission. The military is not purely collectivist; it is a hierarchy that treats certain forms of independence, e.g., moral judgment [3], tactical initiative, and religious accommodation, as useful, while subordinating others to cohesion and readiness.
This distinction is especially clear when governing the body itself. For civilians, our bodies have rights and are generally self-governed. But for our armed forces, their bodies are operational assets, a source of strength or a point of risk.
Secretary Hegseth’s appearance rules are justified by discipline, cohesion, safety, and shared identity. While some accommodations exist, the collective claim is dominant.
Medical autonomy is harder because of conflicting definitions of the body. In the military, the body is both self-owned and part of a collective readiness system. The military does not entirely deny the first claim; it subordinates it when individual refusal is judged to threaten the unit.
The military body acts as a boundary object: simultaneously a rights-bearing individual, a biological system, a point in a disease network, and a tool for national defense. Discussions about vaccines or treatments center on what level of autonomy can persist within an institution designed for collective action. In civilian contexts, public health mandates must compete with stronger assumptions of personal liberty and a broader perception of shared risk.
That is why the contrast between stricter appearance rules and relaxed influenza vaccination requirements is not necessarily hypocritical. It reflects a judgment, correct or not, that different claims on the body carry different readiness consequences. Moreover, the divergence between stricter appearance rules and relaxed influenza vaccination requirements reflects not a simple prioritization but a complex of decisions made under uncertainty—where the effects of medical policy on readiness are indirect and difficult to quantify, and where multiple forms of readiness risk (health, personnel, cohesion) are weighed without definitive comparative data.
Hegseth’s decision may therefore be less a rejection of military collectivism than a narrowing of where the collective claim is asserted. The armed forces still regulate the body extensively. What has shifted is the threshold for compelling medical compliance, particularly when the disease is familiar, recurrent, usually low-severity in the military demographic, and politically entangled with the residue of COVID.
[1] This is based on the levels of infectivity and morbidity during the Revolutionary War.
[2] 153 have returned to service
[3] This is a variant of the controversy over the requirement of members of the armed forces to question and, if necessary, disobey an “illegal order.”

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


