Today, we rank 50th in life expectancy globally and have increasingly diverged from our “high-income” country (HIC) peers. By any measure, we spend more on healthcare than any other wealthy nation. In 2024, we spent, on average, $14,000 per person, more than twice that of #2, Switzerland. While our peers spend roughly 11% of their GDP on healthcare, we spend 17%. We remain a global hub for medical innovation and specialized facilities, with 4 of the top six global medical facilities located in the US. So why these abysmal findings?
To answer this, we must look beyond the price tag and examine the specific metrics of how we are falling behind.
The Math of Loss
A new study in JAMA seeks to quantify the causes of those deaths to “illuminate avenues for prevention.” The bulk of the data comes from the World Health Organization Mortality Database, an aggregate of each nation’s vital registries. 99% of the deaths had a valid, recorded underlying cause.
To understand the scale of this crisis, the study uses three specific measures, including excess deaths—which is simply the difference between the number of deaths observed in the US and the number we would expect if our mortality rates matched those of our peer nations.
Over a 24-year interval, the US experienced 12.6 million of these excess deaths. This staggering figure accounts for 314 million years of birthdays, graduations, and retirements that "never happened" because of preventable deaths, calculated as years of life lost (YLL). Ultimately, this gap resulted in an all-cause mortality rate that was 1.38 times higher than that of our peers. Because deaths at younger ages accrue more YLLs, these metrics reveal that we aren't just dying—we are losing a massive amount of "stolen time".
This massive loss of life follows a “two-part narrative” split between the violent risks facing our youth and the chronic failures affecting the elderly.
A Tale of Two Tragedies
For our younger generation, ages 0 to 44, the majority of excess deaths are driven by external causes: transportation accidents, homicides, and drug poisonings. Our homicide rate is 14.25 times greater than that of our peers, and drug deaths are 7.48 times higher. Deaths of despair—including drug “poisoning,” alcohol-related deaths, and suicides—accounted for 14% of deaths but a disproportionate 22% of YLLs because they primarily affected the young and middle-aged. While the US was near parity with peer nations in 1999 for deaths of despair, the introduction of fentanyl into the drug supply resulted in 131,000 more excess deaths than our peers.
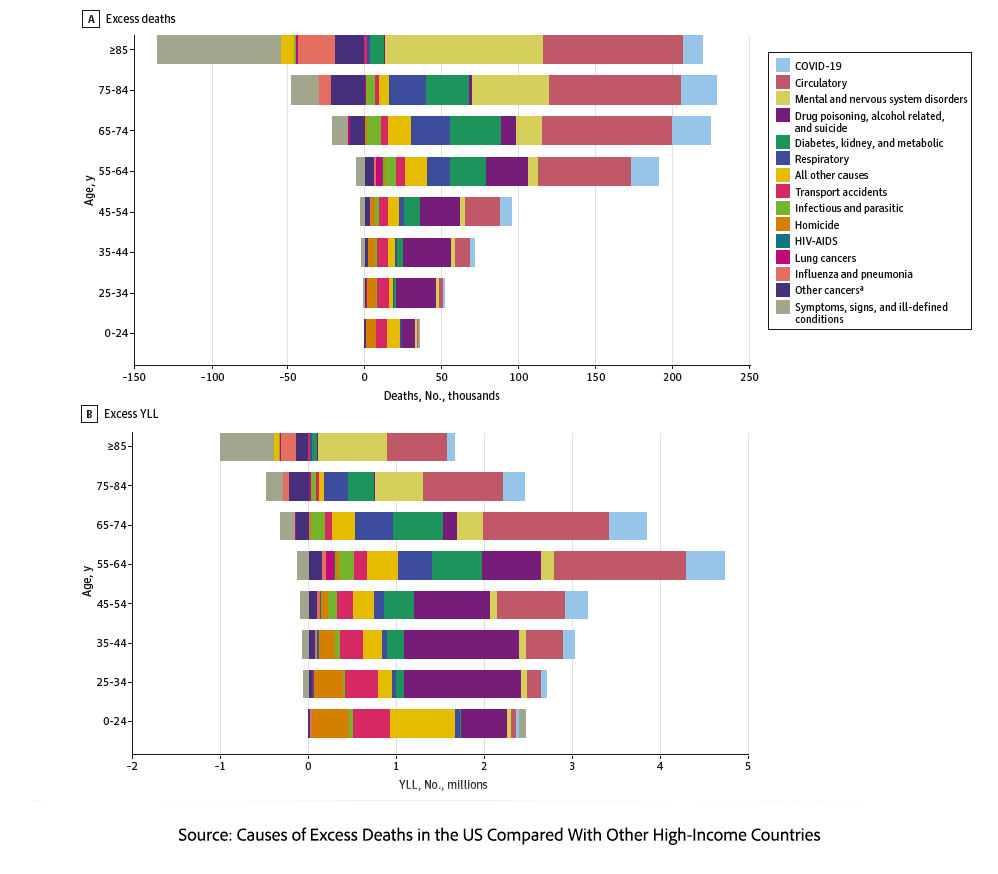
Conversely, midlife and older adults face a steady rise in circulatory and metabolic deaths. Cardiovascular disease, at 40%, remains the single largest contributor to excess deaths, followed by mental and nervous system disorders at 20%. Over the past 24 years, we have seen an earlier onset of diabetes and obesity. During that period, diabetes has moved from the fifth to the third leading cause of death. The earlier onset of obesity, diabetes, and kidney disease among middle-aged adults has led to a rising tide of cardiovascular deaths among them and those 65 or older, resulting in more excess cardiovascular deaths now than 20 years ago. Finally, mental and nervous system illness saw a massive spike in the first decade of the century, the largest increase for any cause. Among the very elderly, aged 85 and older, these disorders are now the leading cause of excess mortality.
These divergent tragedies suggest that our mortality disadvantage is not solely due to a lack of expertise or access, but rather a symptom of our surroundings.
The Broken Environment
Our disadvantage stems from divergent social and economic environments. Socioeconomic drivers, including the loss of manufacturing jobs and automation, have worsened opportunities for those already struggling, while deaths from drugs, alcohol, and suicide remain closely associated with social disadvantage. The "iron law of prohibition" has further ensured that the war on drugs leads to a supply of increasingly potent opioids like fentanyl. Furthermore, we live in a food environment that, for whatever reason, contributes to growing waistlines and metabolic dysfunction from fats and sugars.
Understanding these environmental drivers clarifies why our policy responses are focused on the wrong targets.
A Take-away
Ultimately, this study shows that high-quality clinical care alone is insufficient to counteract the systemic drivers of disease. Despite spending twice as much on healthcare as our closest peer nations, our 50th-place ranking in life expectancy underscores a profound 'mortality disadvantage' rooted in socioeconomic disparity. We are spending more to live less. True prevention is more than an individual monitoring their cholesterol or glucose; it requires a fundamental shift toward improving the environments that shape those health metrics in the first place.
Swapping out food colors, defining ultra-processed food, and increasing paperwork to more carefully screen for medical assistance are all low-hanging fruit of distraction. Our “mortality disadvantage” is not a lack of technology or specialized facilities, nor is it the control of our largesse, but a result of the social and economic environment we allow to persist.
Source: Causes of Excess Deaths in the US Compared With Other High-Income Countries JAMA Network Open OI: 10.1001/jamanetworkopen.2026.6147

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


