
According to STAT, Chris Klomp, the director of the Center for Medicare, “is considering a policy that would automatically enroll Medicare beneficiaries into Medicare Advantage plans,” or into Accountable Care Organization (ACO), another form of value-based risk sharing. Currently, new beneficiaries are given a choice—and if they do not actively choose, they are defaulted into traditional Medicare.
National debates often focus on the economics of these options, but a more revealing approach is to examine what “value” actually means in practice and whether these models deliver on it.
How ‘Value’ Entered Medicare
Value entered Medicare gradually, as a layering of ideas onto a fee-for-service foundation. In the 1980s and 1990s, Medicare began experimenting with shifting financial responsibility to private plans through risk-based payments (the precursors to Medicare Advantage), introducing the idea that spending could be managed in advance rather than reimbursed after the fact. In the 2000s, CMS began to explicitly incorporate the idea of “value” through pay-for-performance programs, which rewarded reporting and, later, performance on quality metrics, although without significant financial penalties.
The Affordable Care Act of 2010 marked a decisive shift. It established Accountable Care Organizations and the Center for Medicare & Medicaid Innovation, formally linking payment to both cost and quality. Shared savings programs became a bridge from incentives to accountability. Today, that framework continues to expand, with CMS aiming for all traditional Medicare beneficiaries—and most Medicaid beneficiaries—to be in accountable care relationships by 2030. [1]
If “value” is now the guiding principle, the next question is what that principle is supposed to achieve.
Who Chooses—Patients or Policy?
“Accountable relationships lead to higher-quality measures, a better clinical experience, better clinical performance. It’s healthier beneficiaries, healthier patients.”
- Chris Klomp, Director of Medicare
As the STAT article continues, the Heritage Foundation’s Mandate for Leadership suggested that Medicare Advantage be the default option for value-based risk sharing. Defaults matter: in one study, 90% of Medicare beneficiaries selecting a drug plan accepted the default option.
The Heritage Foundation’s recommendation was based on four principles:
- “Increase Medicare beneficiaries’ control of their health care. Patients are best positioned to determine the value of health care services, working with their health care providers.
- Reduce regulatory burdens on doctors. Doctors must be free to focus on treating patients first, not entering codes on computers, and should not be tempted to change their medical judgment based on arbitrary or illogical reimbursement incentives.
- Ensure sustainability and value for beneficiaries and taxpayers. … Intermediate entities that can manage financial risk and ensure quality of care are important in transitioning to value-based care within the Medicare program.
- Reduce waste, fraud, and abuse, including through the use of artificial intelligence for their detection.”
These core principles were echoed by the Paragon Health Institute, which STAT describes as a conservative think tank, who went on to add that
“The best way to manage Medicare is to empower beneficiaries to make their own decisions”
[emphasis added]
That emphasis on choice sits uneasily alongside the idea of a default enrollment.
The principles themselves are difficult to dispute. The more important question is whether Medicare Advantage (MA), as currently implemented, actually fulfills them.
Testing the Promise Against Reality
 “Increase Medicare beneficiaries’ control of their health care” In theory, Medicare Advantage emphasizes patient choice, allowing beneficiaries to select plans that match their needs. In practice, however, that control is influenced by network design.
“Increase Medicare beneficiaries’ control of their health care” In theory, Medicare Advantage emphasizes patient choice, allowing beneficiaries to select plans that match their needs. In practice, however, that control is influenced by network design.
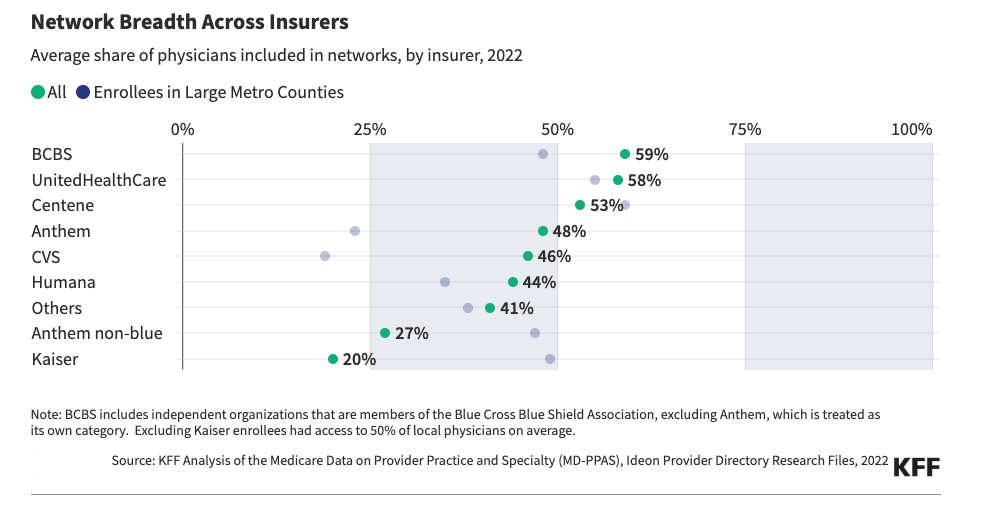
Medicare Advantage plans may offer care coordination and additional benefits, which some beneficiaries value. However, control depends not only on coverage but also on which physicians and hospitals are included. Narrower networks can also limit choice, especially for patients seeking long-term relationships with specific physicians. A study by KFF found that provider networks in MA plans are much narrower than those under traditional Medicare, with significant regional differences—ranging from an average of 18% of eligible providers in San Diego to 58% in Tucson. More importantly, only about 55% of primary care physicians in an area, on average, participate in MA networks.
Overall, this suggests that while MA can coordinate care more efficiently, it might also limit the level of control patients can realistically have.
“Reduce regulatory burdens on doctors.” Another central promise of value-based care is to reduce administrative friction so clinicians can focus more on patient care. Here, the contrast between traditional Medicare and Medicare Advantage is stark.
In traditional Medicare, prior authorization applies to a relatively small set of high-risk services [2], resulting in about 625,000 requests annually—roughly 0.02 per enrollee. Of these, about 23% are denied. In contrast, Medicare Advantage plans processed approximately 53 million prior authorization requests in 2024, or about 1.7 per enrollee, with a denial rate of 7.7%.
This represents an approximately 85-fold increase in the frequency of prior authorization requests. While MA plans argue that these tools help reduce unnecessary care, the scale of their use suggests a system that imposes substantially greater administrative burdens on providers.
Appeals are relatively uncommon in both systems. However, when MA denials are appealed, over 80% are overturned, suggesting that many initially denied services are ultimately considered medically necessary. This pattern suggests that prior authorization might serve less as a safeguard against inappropriate care and more as a way to delay access. In contrast, traditional Medicare’s limited use of prior authorization leads to fewer such delays.
“Ensure sustainability and value for beneficiaries and taxpayers.” A key argument for Medicare Advantage is that proactive care management can reduce overall costs while maintaining or improving quality. The evidence, however, is mixed. Ever since Vice President Gore promised to keep Medicare’s largest revenue source, payroll taxes, in a “locked box,” we have periodically heard that the Medicare Trust Fund is running low. The Congressional Budget Office currently projects that the Medicare Trust Fund will remain solvent through 2040, with spending beginning to outpace revenue after 2031. Within that broader context, MedPAC estimates that the federal government will spend about $84 billion more on Medicare Advantage beneficiaries than on similar individuals in traditional Medicare in 2025 [3], making it harder to see a clear fiscal benefit for taxpayers.
Higher costs may be justified if they consistently lead to better outcomes. However, a report by the Commonwealth Fund found no significant overall difference in the populations served or the quality of care provided. Medicare Advantage outperformed traditional Medicare in certain areas, such as preventive services and hospital readmissions, while traditional Medicare performed better in others, including access to top cancer hospitals and high-quality home health agencies. A KFF meta-analysis of 62 studies reached similar conclusions.
Taken together, the evidence suggests that Medicare Advantage does not consistently deliver superior value when both cost and quality are considered.
“Reduce waste, fraud, and abuse.” Reducing improper payments is another central goal of value-based care. These payments include errors, administrative issues, and fraud, though not all improper payments are fraudulent.
Traditional Medicare has an estimated improper payment rate of 7.7%, compared to 5.6% in Medicare Advantage. On the surface, this suggests an advantage for MA. However, these figures capture different dynamics within each system.
Reducing improper payments is another central goal of value-based care. These payments include errors, administrative issues, and fraud, though not all improper payments are fraudulent.
Traditional Medicare has an estimated improper payment rate of 7.7%, compared to 5.6% in Medicare Advantage. On the surface, this suggests an advantage for MA. However, these figures capture different dynamics within each system.
A significant portion of Medicare Advantage spending—estimated at roughly $40 billion of the $84 billion in excess payments—has been linked to coding intensity, or “upcoding,” where higher risk scores result in higher payments. Whether this reflects deliberate manipulation or the structure of incentives remains contested. What is clearer is that these payment differences significantly add to overall program costs. MA does not necessarily translate into lower total spending or greater efficiency.
When Policy Becomes Reality
According to Becker’s Payer Issues, the big six health insurers already control health care coverage for 181 million people in the US. The potential default nudge by Chris Klomp could add another 33 million.
Ultimately, the debate over defaulting beneficiaries into Medicare Advantage isn't really about ideology or economics—it centers on whether the current implementation of value-based risk sharing achieves its intended goals. The term “value” promises autonomy, efficiency, and better outcomes, but real-world experience reveals a more complicated trade-off: narrower networks instead of wider choices, more administrative hurdles rather than fewer, and higher overall costs despite claims of efficiency.
Defaults are so influential because they bypass detailed discussion, turning policy choices into patient realities. Before moving millions of beneficiaries through such a nudge, the evidence should show that Medicare Advantage consistently delivers on its promises—not just in theory, but in real practice. Until then, the question isn’t so much whether value-based care is desirable, but whether Medicare Advantage, as it exists today, is the right way to provide it—or if we’re just redefining the term “value” to fit the system we already have.
[1] Currently, just over 53% of Medicare beneficiaries are enrolled in accountable care arrangements.
[2] The 70 “high-risk” services included durable medical devices (e.g., mobility devices and prosthetics); hospital outpatient care for cosmetic-related services; some high-cost, low-value procedures (e.g., spinal neurostimulators, cervical fusion, and facet joint interventions); and repetitive non-emergent ambulance use.
[3] MedPAC reports that these higher costs result from “favorable selection,” where beneficiaries have lower actual spending compared to payments based on “risk scores,” and from “coding intensity,” which lead to higher risk scores and payments after Medicare Advantage upcodes their risk.

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


