A Year-Long Plan for Lifestyle Change
The Medicare Diabetes Prevention Program (MDPP)—the first preventive service model tested by CMS—promotes lifestyle changes, especially weight loss and increased physical activity, among beneficiaries at heightened risk for developing Type II diabetes. The program reflects MAHA’s broader push for health-system transformation, prioritizing preventive care and expanding the range of people and organizations that can deliver it.
The program was open to all beneficiaries, including those enrolled in “traditional” and Medicare Advantage plans. Eligible beneficiaries, most often referred by their physicians when a heightened risk was acknowledged (by being overweight or an elevated HbA1c), underwent a year-long program in which the initial 16 “core sessions focused on changing eating habits and encouraging physical activity.” The sessions, led by lifestyle coaches, included follow-up maintenance sessions and were delivered both in person and virtually. Participants were weighed at each session. The outcomes of interest were a weight loss of 5% or more of original body weight and delaying or preventing the onset of diabetes. [1]
Seven Years of Tweaks and Revisions
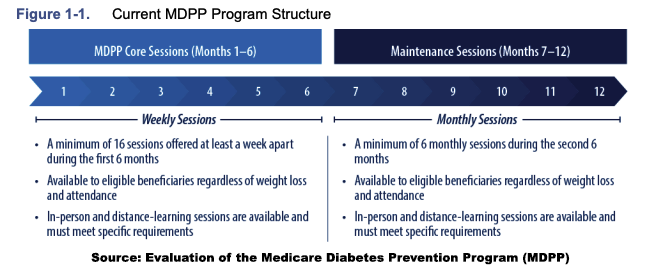
These foundational details set the stage for understanding how the program evolved. The program changed from its original form over the next 7 years, loosening requirements on beneficiaries, initiating virtual visits in the face of COVID, eliminating hurdles to supplier participation, and adjusting payments to reflect a one-year, not two-year program
Provider Landscape
The program’s expanded provider landscape included traditional healthcare organizations, state and local health departments, and community-based groups such as YMCAs and wellness centers. These suppliers operated an average of four program sites each. Although traditional healthcare organizations delivered about two-thirds of all sessions, community-based groups accounted for roughly half of the program locations, giving them a disproportionately larger, more local geographic footprint.
Overall, 357 suppliers provided the program at 1,370 sites. However, the geographic dispersion of the program was not uniform, more often in the Northeast, with “a notable lack of delivery sites in the Mountain West and Sunbelt regions.” The highest prevalence of diabetes is in the Southern US, with the most suppliers in the areas with lower than the national average prevalence of diabetes and obesity. Based on zip code data, two-thirds of participants lived within 25 miles of their program site. As would be expected, beneficiary participation declined as distance from participating sites increased. Interestingly, contrary to what might be anticipated, beneficiaries utilizing virtual visits showed nearly identical drop-offs with distance.
A Reimbursement Problem
The payment process was described as making “it difficult to focus on recruitment, as a good deal of staff time is dedicated to billing, submitting reports, and coding claims.” [2] Claims were submitted for about two-thirds of participants, and CMS reimbursed suppliers for only 37% of those claims (24% is the aggregated total). The program's maximum potential payment was about $770 per beneficiary. Suppliers received an average of $283 per beneficiary, about a quarter of which was for meeting target weight-loss goals, and the rest for meeting attendance targets.
The Beneficiaries - Understanding the Enrolled
Roughly 9,000 beneficiaries enrolled, split evenly between traditional Medicare and Medicare Advantage. Sixty percent of referrals in FFS came directly from physicians, compared with 40% in MA plans—suggesting that MA organizations may rely more heavily on non-physician clinicians for referrals. Physician referrals appeared to matter: 60% of beneficiaries referred by physicians completed the program, compared with a 40% completion rate among those referred by other sources.
Beneficiaries indicated that the primary motivation for participating was their physician (50%), followed by an abnormal blood test. As might be anticipated, MA beneficiaries reported greater motivation by their insurer. Most beneficiaries enrolled to “improve their health,” especially regarding diabetes, and others found weight-loss benefits. Most beneficiaries were women aged 65 to 74, attending on average 18 sessions. 40% of participants paused or discontinued participation.
Interviews with beneficiaries further reveal what helped them stay engaged. Attendance was facilitated by accountability and support, along with structured weekly sessions.
- Individuals “described feeling connected with other beneficiaries,” facilitating the sharing of ideas, tangible successes, e.g., weight loss or reduction in HbA1c levels, and failures, increasing the feeling that they were not alone.
- Realistic lifestyle changes, focused “holistically” on both diet and exercise, are empowered by teaching them to make informed choices and practical ways to change. Tracking food and exercise, while challenging, was facilitated by group-inspired accountability.
- An enthusiastic, supportive, nonjudgmental lifestyle coach who “exhibited accommodating behavior, tailoring advice and feedback to meet their specific needs, and advocated for their health without criticism or shame.”
Outcomes: Weight Loss, Activity, and Habits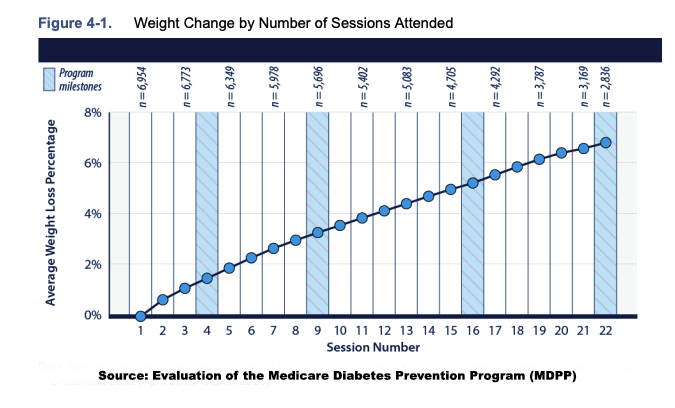
These supportive elements translated into measurable—though uneven—outcomes.
- Weight loss increased with greater attendance. The average loss was 4.9% of starting weight, rising to 6.6% among those who completed the program; those attending fewer than eight sessions lost about 2.9%. Men lost slightly more than women, and physician-referred participants lost somewhat more than those referred through other channels. Half of all participants met the 5% weight-loss goal, and 24% achieved at least 9%. 80% of those who reached 5% maintained it.
- Nearly all beneficiaries self-reported meeting a goal of 150 minutes of physical activity per week (72 and about half said the program helped them establish lasting exercise habits.
- Nutrition education on diet and glucose metabolism, as well as the “plate” approach to nutritional choices, empowered beneficiaries to report “increasing consumption of vegetables, being cognizant of portion sizes, eating more fruits, purchasing healthier snacks, and eating fast food less often.”
No One Enrolled
Only 0.01% of eligible beneficiaries enrolled in MDPP, creating a substantial selection bias that limits comparisons with control groups and prevents generalizing these outcomes to the broader Medicare population [4]. Participants were disproportionately female, motivated by concerns about obesity, and already engaged in preventive health behaviors, like flu vaccination and cancer screenings. Metformin, a drug used in the early treatment of diabetes, is often prescribed off-label to mitigate prediabetes. Eleven percent were taking metformin, compared with none in the control group, further evidence that enrollees differed meaningfully from nonparticipants.
Did MDPP Work?
The true goal was to reduce the incidence of diabetes in this at-risk group. Fifteen percent of MDPP participants eventually received a diabetes diagnosis, roughly in line with expected annual progression rates. Those who achieved at least 5% weight loss progressed somewhat less often, though the difference was not statistically significant. Comparisons with other national DPP efforts, which report progression rates of 4.8–5.3% in treatment groups, further illustrate how methodological differences make direct comparisons uncertain. Overall, the evidence for the impact on diabetes prevention is inconclusive.
The Larger Lesson About Preventive Care
“Although MDPP’s association with weight loss is promising, the reach of the MDPP has been limited.”
That is from the discussion of the MDPP and seems to both oversell the benefit and undersell the limitation. It is better characterized as one of the researchers involved in diabetes prevention efforts describes to MedPage as “pathetic.” It should serve notice to MAHA’s warriors that good intentions and medical freedom to empower the patient/consumer are insufficient. This program faced significant hurdles in implementation, including
- Limited, labor and time-intensive, reimbursement
- An exceedingly low participation rate, consistent with the uptake of other Medicare-covered preventative services, e.g., alcohol misuse or weight counseling, has a participation rate of 1%. The annual Medicare “wellness visit” has a claim rate of approximately 3.7%.
- Social Determinants of Health, including the cost of nutritious food, work obligations limiting available time to participate, transportation costs, and distance, restrict access.
The most crucial hurdle remains insufficient personal motivation. MAHA’s warriors, as is the case for many researchers, are trapped in an echo chamber where everyone is as concerned and engaged on an issue as they are. If nothing else, this program demonstrates the fallacy of that belief. As researchers have found countless times, when their programs are scaled up from carefully curated studies to population health, real-world results can be a bitch.
[1] Matched beneficiaries who did not participate in the program served as the statistical control group.
[2] Initially, suppliers had to provide 15 separate codes to document the beneficiary’s “journey” and care provided. It was simplified to six. These billing difficulties also explain why the two-year program was truncated to one, with all payments shifted into that timeframe.
[3] “defined as those who attended at least eight sessions in the first 6 months and an additional session after Month 6.”
[4] MDPP beneficiaries were compared with 9 million FFS beneficiaries who were potentially eligible due to a prediabetes diagnosis.

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


