Our increasingly busy lives are often sustained, at least in theory, by multitasking—rapidly switching attention between tasks rather than doing them truly in parallel or completing them one at a time. Despite the belief that this boosts productivity, scientific evidence suggests it carries measurable costs.
Each task we perform requires a distinct mental configuration of relevant rules, sensory filters, and objectives.
When we switch our mental gears, we disengage from the old pattern, reconfigure the rules and filters of our mental spaces, and engage with the new setup. Psychologists call the resulting slowdown and increased error rate “task-switch costs.” In addition, the previous task can linger in the background, a phenomenon researchers describe as “cognitive residue” or “task-set inertia,” making it harder to fully focus on what comes next.
There is a different mindset for answering an email than for performing brain surgery. And that provides a neat segue into a study examining task switching among transplant surgeons. The researchers describe organ transplantation as “a natural experiment to measure the impact of task switching,” primarily because donor offers occur unpredictably and there is only a short window in which they can be successfully transplanted. As a result, the transplant surgeon’s scheduled day of procedures can be altered on short notice, and the type of organ being transplanted can change.
Using national transplantation data on abdominal transplants (i.e., kidney, pancreas, small bowel, and liver), the researchers compared outcomes when surgeons switched from one organ type to another (for example, liver to kidney) with outcomes when they repeated the same procedure.
When Switching Becomes Risky
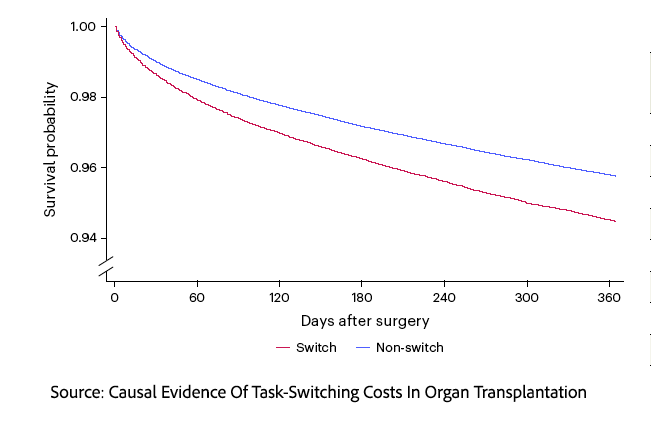 They found a statistically significant increase in 1-year post-transplant mortality in cases where the second transplantation involved a different organ type. I should caution that the 1-year mortality for transplantation is low, at 4.45%, and that the increased mortality raises it to about 5%. This represents a 14.8% relative increase and should draw our attention.
They found a statistically significant increase in 1-year post-transplant mortality in cases where the second transplantation involved a different organ type. I should caution that the 1-year mortality for transplantation is low, at 4.45%, and that the increased mortality raises it to about 5%. This represents a 14.8% relative increase and should draw our attention.
The authors considered several alternative explanations:
- Surgeons operating outside the organ they primarily treat. However, mortality was similarly elevated when they switched back to their primary organ, so unfamiliarity cannot explain the effect.
- More urgent or higher-risk cases. Yet even after adjusting for these factors, the switching effect persisted, indicating that baseline risk was not driving the result.
- Resource constraints from lower staffing on nights and weekends. Again, when controlling for time of day and week, the mortality effect is unchanged.
Taken together, the findings are consistent with a task-switching cost, though—as with any observational study—causality cannot be definitively established. The researchers also identified factors that appeared to reduce the effect. Longer gaps between surgeries diminished the difference, with no significant impact after a day or more. Greater experience helped as well: surgeons with higher case volumes or broader procedural backgrounds showed smaller increases in mortality after switching. Finally, switching between more similar procedures reduced the apparent risk.
It is well established that more experienced surgeons achieve better outcomes, a finding supported by this study. From a practical standpoint, the researchers estimated that 60% of the outcome difference between high- and low-volume transplant surgeons was attributable to a switching effect that might be addressed through surgical scheduling.
Rethinking Surgical Schedules
Designing the daily surgical schedule is an artful dance among surgical, anesthesia, and nursing resources, patient needs, and each surgeon’s idea of their best “workflow.” There is already good evidence that operating rooms are more efficient when a surgeon performs a similar set of procedures on the same day. Some centers have dedicated schedules in which “multi-organ surgeons are assigned to cover a single organ type (kidney or liver) during a given on-call block.” Other centers, often with fewer resources (surgical wants rarely become less), are more flexible, and “the on-call surgeons may handle either organ type within the same block.” The researchers found that center-based mortality was lower in the dedicated centers, where switching was less, suggesting that controlling this cognitive burden may have real-world effects, or, as they write, “scheduling patterns that reduce switching rates are also linked to improved patient survival.”
The Limits of Multitasking
The evidence is hard to dismiss, even in the high-stakes world of organ transplantation. Simply shifting between organs for transplantation can increase mortality, a stark reminder that cognitive limits are unyielding. Our cultural fixation on multitasking treats attention as infinitely divisible, yet it is fragile, sequential, and costly to reconfigure. If we are serious about performance, whether in medicine, business, or daily life, the lesson is not to do more at once but to design our work and expectations around the simple truth that doing one thing well still beats doing many things poorly.
Source: Causal Evidence Of Task-Switching Costs In Organ Transplantation Nature Human Behavior DOI: 10.1038/s41562-026-02459-8

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


